Abstract
Background: The aim of this systematic review and meta-analysis was to compare the clinical efficacy of the early dental implant placement protocol with immediate and delayed dental implant placement protocols.
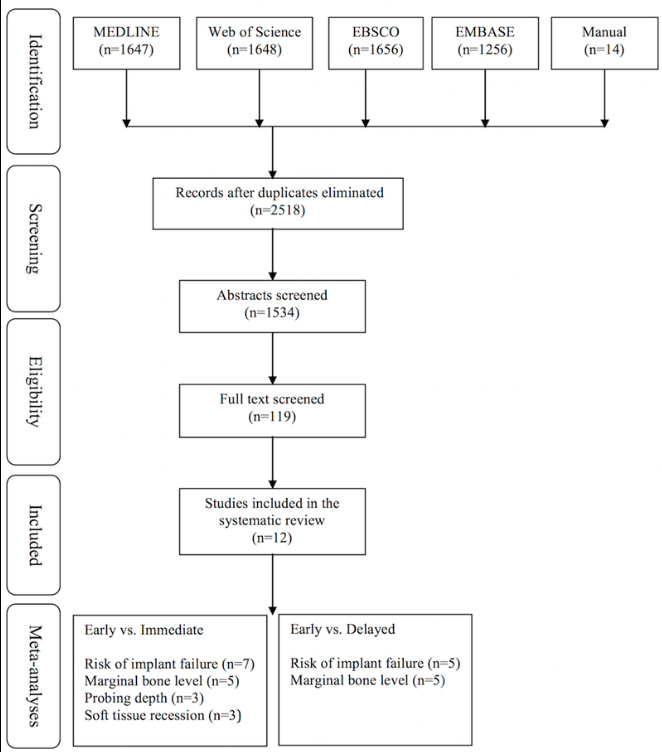
Methods: An electronic and manual search of literature was made to identify clinical studies comparing early implant placement with immediate or delayed placement. Data from the included studies were pooled and quantitative analyses were performed for the implant outcomes reported as the number of failed implants (primary outcome variable) and for changes in peri-implant marginal bone level, peri-implant probing depth, and peri-implant soft tissue level (secondary outcome variables).
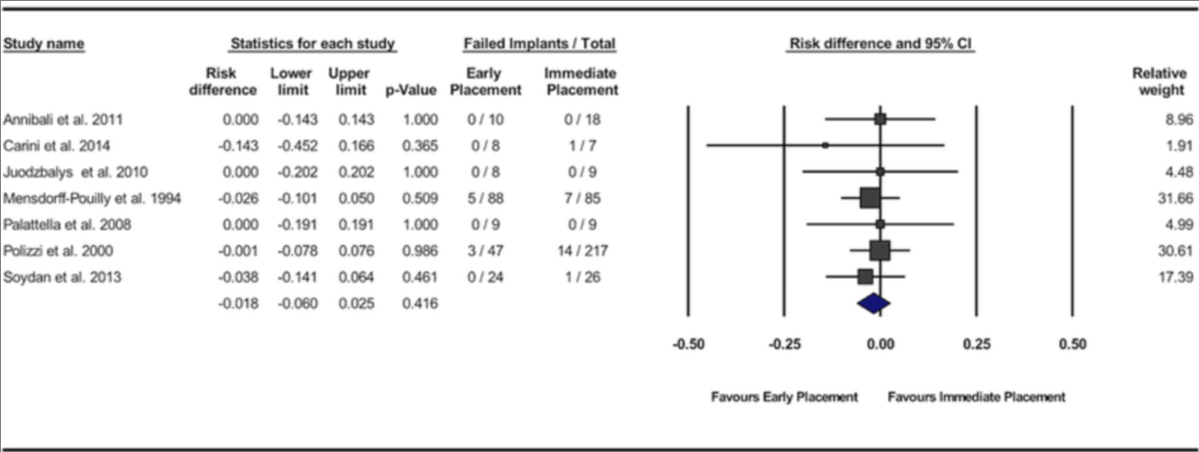
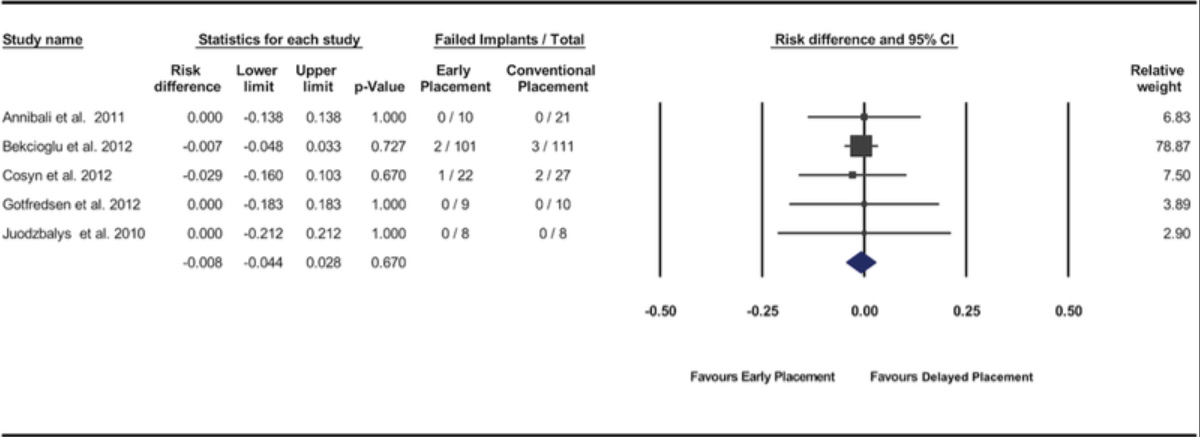
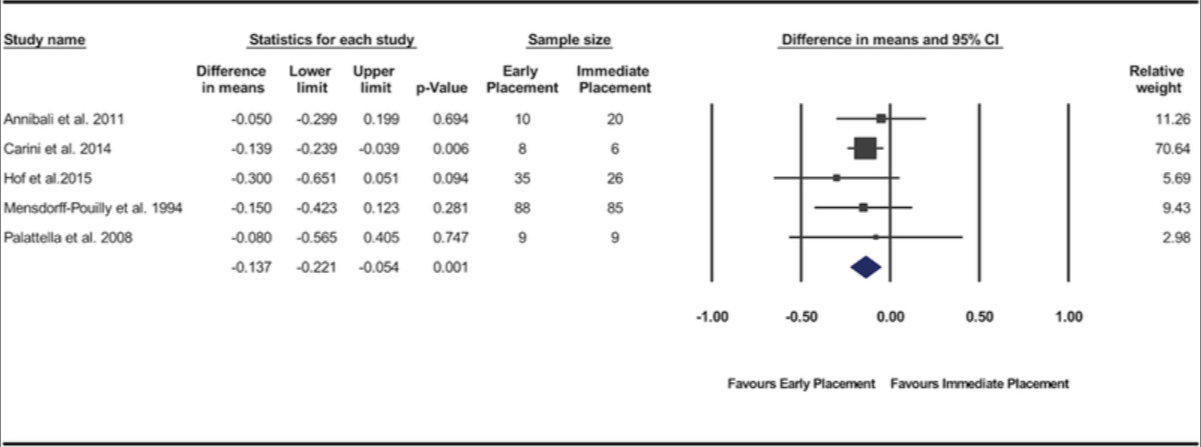
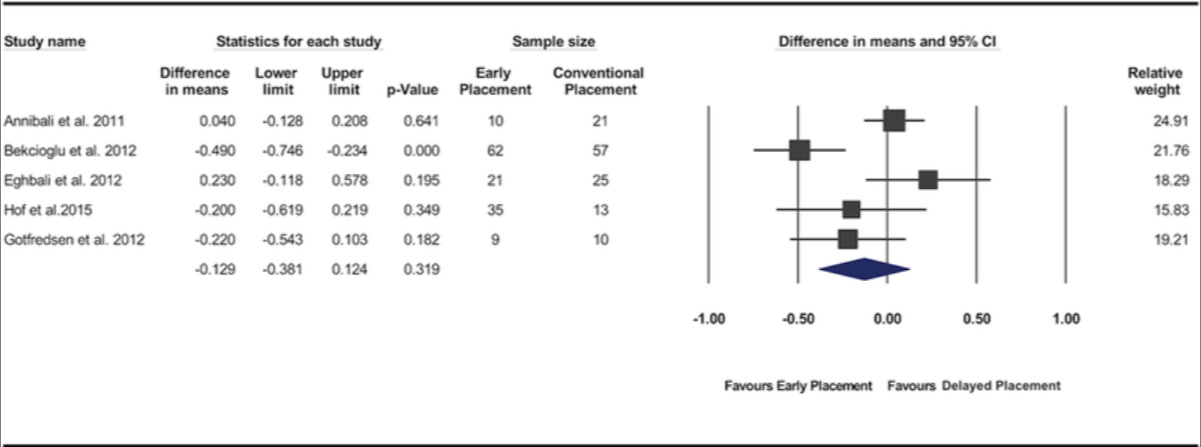
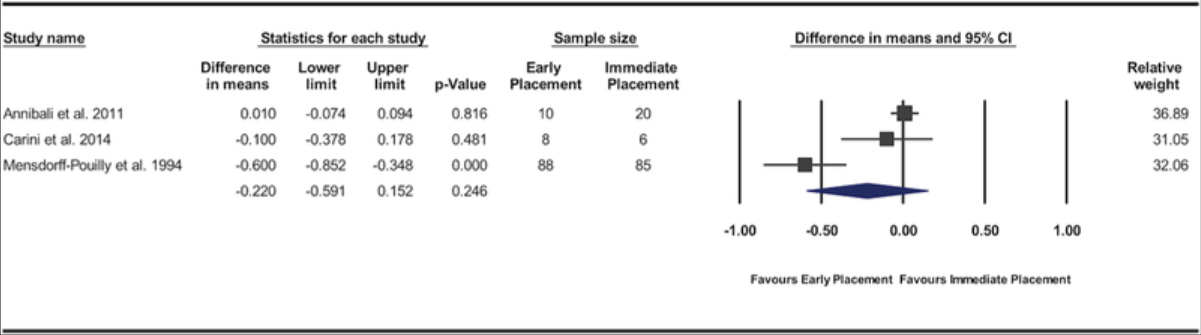
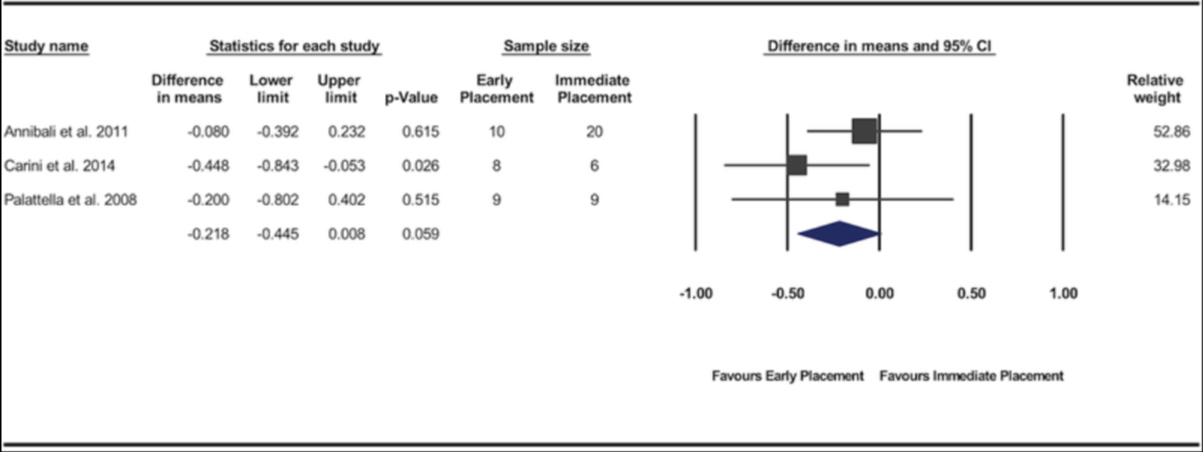
Results: Twelve studies met the inclusion criteria. Significant difference in risk of implant failure was found neither between the early and immediate placement protocols (risk difference = -0.018; 95% confidence interval [CI] = -0.06, 0.025; P = 0.416) nor between early and delayed placement protocols (risk difference = -0.008; 95% CI = -0.044, 0.028; P = 0.670). Pooled data of changes in peri-implant marginal bone level demonstrated significantly less marginal bone loss for implants placed using the early placement protocol compared with those placed in fresh extraction sockets (P = 0.001; weighted mean difference = -0.14 mm; 95% CI = -0.22, -0.05). No significant differences were found between the protocols for the other variables.
Conclusions: The available evidence supports the clinical efficacy of the early implant placement protocol. Present findings indicate that the early implant placement protocol results in implant outcomes similar to immediate and delayed placement protocols and a superior stability of peri-implant hard tissue compared with immediate implant placement.
Keywords: clinical protocols; dental implantation/methods; dental implants; meta-analysis; time factors; tooth extraction; tooth socket/surgery.
Figures
karim El Kholy - Wismeijer D, Joda T, Flügge T, Fokas G, Tahmaseb A, Bechelli D, Bohner L, Bornstein M, Burgoyne A, Caram S, Carmichael R, Chen CY, Coucke W, Derksen W, Donos N, El Kholy K, Evans C, Fehmer V, Fickl S, Fragola G, Gimenez Gonzales B, Gholami H, Hashim D, Hui Y, Kökat A, Vazouras K, Kühl S, Lanis A, Leesungbok R, van der Meer J, Liu Z, Sato T, De Souza A, Scarfe WC, Tosta M, van Zyl P, Vach K, Vaughn V, Vucetic M, Wang P, Wen B, Wu V.
2018 October - Clin Oral Implants Res.
Group 5 ITI Consensus Report: Digital technologies
Abstract
Objectives: Working Group 5 was assigned the task to review the current knowledge in the area of digital technologies. Focused questions on accuracy of linear measurements when using CBCT, digital vs. conventional implant planning, using digital vs. conventional impressions and assessing the accuracy of static computer-aided implant surgery (s-CAIS) and patient-related outcome measurements when using s-CAIS were addressed.
Materials and methods: The literature was systematically searched, and in total, 232 articles were selected and critically reviewed following PRISMA guidelines. Four systematic reviews were produced in the four subject areas and amply discussed in the group. After emendation, they were presented to the plenary where after further modification, they were accepted.
Results: Static computer-aided surgery (s-CAIS), in terms of pain & discomfort, economics and intraoperative complications, is beneficial compared with conventional implant surgery. When using s-CAIS in partially edentulous cases, a higher level of accuracy can be achieved when compared to fully edentulous cases. When using an intraoral scanner in edentulous cases, the results are dependent on the protocol that has been followed. The accuracy of measurements on CBCT scans is software dependent.
Conclusions: Because the precision intraoral scans and of measurements on CBCT scans and is not high enough to allow for the required accuracy, s-CAIS should be considered as an additional tool for comprehensive diagnosis, treatment planning, and surgical procedures. Flapless s-CAIS can lead to implant placement outside of the zone of keratinized mucosa and thus must be executed with utmost care.
karim El Kholy - El Kholy K, Freire M, Chen T, Van Dyke TE.
2018 June - Front Immunol.
Resolvin E1 Promotes Bone Preservation Under Inflammatory Conditions
Abstract
Resolvins are endogenous lipid mediators derived from omega-3 fatty acids. Resolvin E1 (RvE1), derived from eicosapentaenoic acid (EPA), modulates osteoclasts and immune cells in periodontal disease models. The direct role of RvE1 in bone remodeling is not well understood. The objective of this study was to determine the impact of RvE1 on bone remodeling under inflammatory conditions. Our working hypothesis is that RvE1 downregulates bone resorption through direct actions on both osteoblast and osteoclast function in inflammatory osteoclastogenesis. A tumor necrosis factor-α induced local calvarial osteolysis model with or without the systemic administration of RvE1 was used. To evaluate osteoclastogenesis and NFκB signaling pathway activity, murine bone tissue was evaluated by Micro CT (μCT) analysis, TRAP staining, and immunofluorescence analysis.
Mechanistically, to evaluate the direct role of RvE1 impacting bone cells, primary calvarial mouse osteoblasts were stimulated with interleukin (IL)-6 (10 ng/ml) and IL-6 receptor (10 ng/ml) and simultaneously incubated with or without RvE1 (100 nM). Expression of receptor activator of NFκB ligand (RANKL) and osteoprotegerin (OPG) was measured by ELISA. RNA sequencing (RNA-Seq) and differential expression analysis was performed to determine signaling pathways impacted by RvE1. The systemic administration of RvE1 reduced calvarial bone resorption as determined by µCT.
Histologic analysis of calvaria revealed that osteoclastogenesis was reduced as determined by number and size of osteoclasts in TRAP-stained sections (p 0.05). Immunofluorescence staining of calvarial sections revealed that RvE1 reduced RANKL secretion by 25% (p 0.05). Stimulation of osteoblasts with IL-6 increased RANKL production by 30% changing the RANKL/OPG to favor osteoclast activation and bone resorption. The ratio changes were reversed by 100 nM RvE1. RvE1 decreased the production of RANKL maintaining an RANKL/OPG more favorable for bone formation. RNA-Seq and transcriptomic pipeline analysis revealed that RvE1 significantly downregulates osteoclast differentiation mediated by differential regulation of NFκB and PI3K-AKT pathways.
RvE1 reduces inflammatory bone resorption. This action is mediated, at least in part, by direct actions on bone cells promoting a favorable RANKL/OPG ratio. Mediators of resolution in innate immunity also directly regulate bone cell gene expression that is modulated by RvE1 through at least 14 specific genes in this mouse model.
karim El Kholy - Kholy KE, Genco RJ, Van Dyke TE.
2015 June - Trends Endocrinol Metab.
Oral infections and cardiovascular disease
Abstract
Oral infections are the most common diseases of mankind. Numerous reports have implicated oral infections, particularly periodontitis, as a risk factor for atherosclerotic cardiovascular disease (CVD). In this review we examine the epidemiology and biologic plausibility of this association with an emphasis on oral bacteria and inflammation. Longitudinal studies of incident cardiovascular events clearly show excess risk for CVD in individuals with periodontitis. It is likely that systemic exposure to oral bacteria impacts upon the initiation and progression of CVD through triggering of inflammatory processes. Given the high prevalence of periodontitis, any risk attributable to future CVD is important to public health. Unraveling the role of the oral microbiome in CVD will lead to new preventive and treatment approaches.
karim El Kholy - Anderson LE, Inglehart MR, El-Kholy K, Eber R, Wang HL.
2014 August - Implant Dent.
Implant associated soft tissue defects in the anterior maxilla: a randomized control trial comparing subepithelial connective tissue graft and acellular dermal matrix allograft
Abstract
Introduction: This randomized controlled clinical pilot trial compared the efficacy of 2 soft tissue grafting methods for correcting esthetic discrepancies associated with definitively restored implant crowns.
Methods: Thirteen patients presenting with implants displaying recession, thin biotype, concavity defects, or a combination thereof associated with single crowned dental implants randomly received subepithelial connective tissue grafts (SCTG) in the control group (N = 7) or acellular dermal matrix (ADM) allografts in the test group (N = 6), both under coronally positioned flaps. Data regarding soft tissue, hard tissue, esthetics, and quality of life (QoL) parameters were collected over 6 months.
Results: Both groups gained tissue thickness (SCTG: 63% and ADM: 105%), reduced concavity measures (SCTG: 82% and ADM: 96%), and improved recessions (SCTG: 40% and ADM: 28%) from baseline to 6 months. Clinicians determined improvement in esthetics for both groups (P = 0.001), unlike patients who did not change their esthetic ratings. No statistical differences were noted for QoL assessment; however, ADM subjects had more eventful wound healing (P = 0.021).
Conclusions: Within the limitations of this study, both SCTG and ADM result in increased mucosal thickness, reduction in concavity dimensions, and have a potential for recession reduction on definitively restored dental implants.
karim El Kholy - Chan HL, El-Kholy K, Fu JH, Galindo-Moreno P, Wang HL.
2010 December - Implant Dent.
Implant primary stability determined by resonance frequency analysis in surgically created defects: a pilot cadaver study
Abstract
Aim: Implant primary stability is a prerequisite for implant success. A dehiscence or a circumferential defect (CD) at the time of implant placement presents a challenge for achieving primary stability. The aim of this study was to examine the correlations between implant primary stability determined by resonance frequency analysis (RFA) and periimplant bone levels.
Materials: Ten implants were placed in 2 cadaver heads. A series of different sizes of narrow (NDD) and wide (WDD) dehiscence defects and CDs were surgically created around 6 and 4 implants, respectively. Implant primary stability in each size of the 3 different defect types was measured with RFA. For each defect type, the association between the RFA readings and the defect size was plotted and statistically analyzed.
Results: In NDD study, the RFA readings were not correlated with the defect size. In WDD study, the association was significant for most implants, with the coefficient correlation (r) ranging from -0.88 to -0.97. In CD study, there was also a significant association between the implant stability quotient readings and the bone levels, and the r ranged from -0.94 to -0.99.
Conclusion: The association between implant primary stability measured by RFA and the size of surrounding bone defects was defect type dependent. The correlation was highly significant for WDD and CD but not for NDD.